



{kind=link}

Why was the distinguishing mark of female genitalia erased from NASA’s 1970s image travelling outer space? And will compromised depictions of life on Earth avoid sexist, racist and anthropocentric simplifications by 2036?
The commercialized celebration of minority groups distracts from real social and economic issues. Rainbow-washing can veil persistent homophobia, while ‘clapping for carers’ obscures the hardships health sector workers face.
Just four decades ago, young men were dying in secluded hospital rooms. Saying a final farewell to loved ones was strictly forbidden. A year or so earlier, many of them had been fit and well, surrounded by friends and loved ones. Now they were shut into single, inpatient rooms, isolated and at worst completely abandoned.
The bedridden gay man, ill with AIDS, became a well-established image in narratives of the time, and familiarity has not made his story any less painful. He had been deserted for a range of reasons. One was that those close to him were fearful as well as ignorant of virus transmission routes, and stayed away in consequence. The effect was to sequester the dying, sometimes even in the last hours of their lives, and separate them from their closest companions. Hostile families often added to everyone’s misery by ensuring that friends and lovers were excluded from funeral services.
One by one, lives were extinguished and life stories dismissed and lost. Eventually, a majority of people, many of them previously non-activists, voiced their despair to rouse the politicians who had so long refused to listen.
Today we are witnessing the global spread of a new infectious disease. Once again, people are dying alone, in technically advanced capsules lined up in intensive care units, or in the single rooms of care homes, each cell pared down to an inhuman minimum. The isolation measures have more rational motives than in the past, since we have a reasonably good grasp of how the new virus is transmitted.
In the days of the HIV pandemic, social distancing was practised for very mixed motives. It reflected levels of ignorance about how the virus spread and intense distaste for a widely despised form of sexuality. Today, isolation must be acknowledged as a commendable practice, at least in the sense that it is a defence against visitors passing the infection on to others.
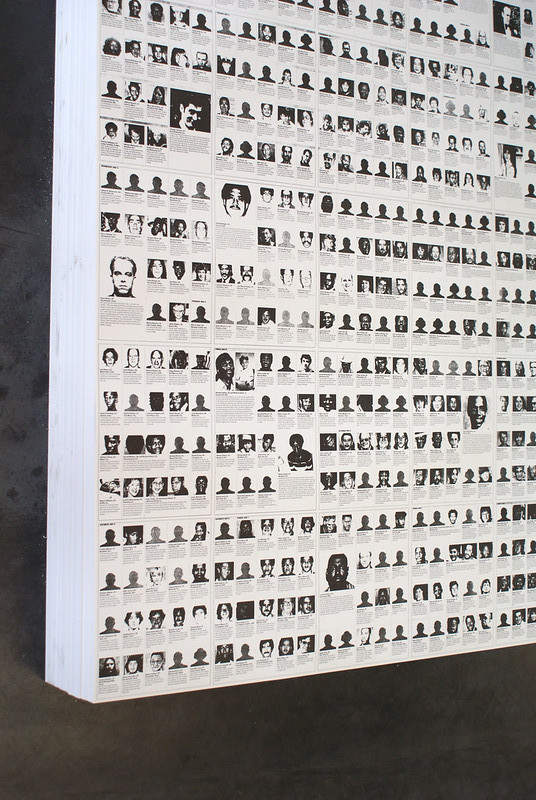
Felix Gonzalez-Torres, ‘Specific Objects without Specific Form’ retrospective at Wiels, February 2010. Photo by Marc Wathieu.
The evidence base for excluding the dying from their previous existence may offer some small comfort, even though allowing people to die with no one at their side is nothing short of heart-breaking.
Parallels between AIDS and COVID-19 have been widely noted. In the Swedish magazine Ottar, Tomas Hemstad asks what lessons from the AIDS crisis might be applicable now, as we endure the spread of COVID-19.1 It is a good question.
While some aspects of the two pandemics are similar, many differ radically. The transfer of infection then and now has followed chronologically recognisable patterns, and this drives the process of re-examining and comparing past and present. In both instances, the upgrading of an epidemic to a pandemic, the initial uncertainty about transmission routes and prognoses for the illness coincided with wide-spread horror at the indiscriminate and unexpected way the infection struck.
When, in March 2020, Madonna called COVID-19 ‘a great equalizer’ on Instagram, she gave voice to a wide-spread initial response to the illness. She meant, of course, that the virus infected poor and rich alike. But since she was immersed in a bath scattered with rose petals at the time, her post became notorious for its insensitivity.2
The clip of Madonna philosophising in her bathtub was quickly taken down, partly because of the scorn poured upon it, but perhaps also because it soon became abundantly clear that the epidemic didn’t affect everyone in the same way. Marginalized groups had the worst experiences.
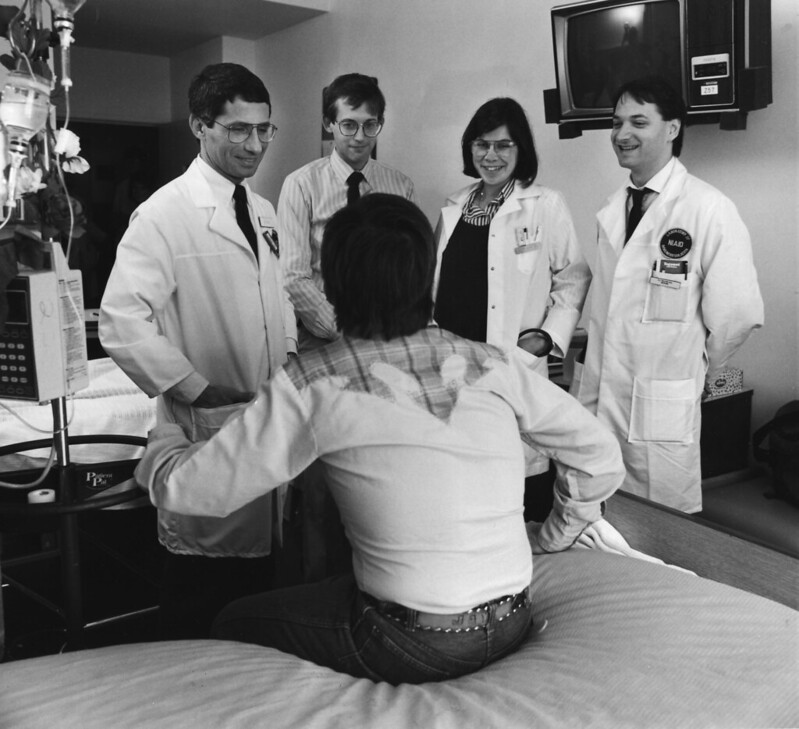
Dr. Anthony Fauci and his team with an early AIDS patient at NIH, 1987. Photo by NIAID from Flickr.
Before AIDS (Acquired Immune Deficiency Syndrome) became the accepted acronym in the United States, other abbreviations had been in circulation. They included GRID (Gay-Related Immune Deficiency) and 4H disease, with each ‘H’ referring to an allegedly high-risk group: Haitians, homosexuals, haemophiliacs and heroin addicts. In other words, the AIDS crisis produced numerous examples of an epidemiological approach based on identifying risk-groups. Consequently, these groups were stigmatized.
There are also other problems inherent in risk-group thinking, which can compromise work on tracing the infection and protecting against it. For example, a majority without risk identifiers may feel a false sense of security and consider themselves exempt from guidelines on how to protect themselves and others. The risk-group approach could even lead to a revision of the social significance of the disease and to the conclusion that it does not merit a community-wide eradication effort.
During the early years of the AIDS epidemic, the central problem was precisely that the worst afflicted group was believed to consist of people deemed unworthy of serious attention. It followed that public health experts need not give it too much time.
Because the disease was closely associated with male homosexuality, and gay sexual behaviour was seen as the critical factor in the spread of infection, it was barely mentioned by the leading politicians of the day. In the USA, four long years passed before president Ronald Reagan could even bring himself to name-check the disease.3 He finally spoke about it in September 1986, after many had suffered and died.
If HIV had been spreading among those closer to the corridors of power, would the research effort have moved faster? Would active antiretroviral drugs have been developed sooner? Might we have found a cure by now?
In contrast, lack of recognition seems less of an issue in the current pandemic. The fact that COVID-19 is especially dangerous for older people may have been reflected in the relatively ineffectual interventions put in place to stop the spread of infection. Perhaps such measures would have been better planned and investigated more vigorously if those worst affected had been young or middle-aged. Nonetheless, COVID-19 is presented as a greater risk to society as a whole.
It is difficult, therefore, to discuss parallels between the frameworks of recognition given to groups hardest hit by HIV/AIDS in the 1980s and by coronavirus in the current pandemic. How should we approach a comparison between these two processes of recognition? What did recognition imply then, and what does it mean now?
The AIDS crisis made it clear that lack of recognition can lead to an intensification of suffering. This essay does not propose to focus only on the risks of denial, however. It also aims to investigate two expressions of recognition that can easily prompt erroneous responses: ‘empty’ recognition and ‘misleading’ recognition.
The first of these refers to insubstantial symbolic words or acts with no real anchorage, which are of no benefit to anyone except possibly the originator. The second – ‘misleading’ recognition – refers to the expression of socially acceptable sentiments to achieve political goals that are unrelated to them.
The latter variant can prove especially treacherous and lead to particularly negative outcomes. As frameworks, both ‘empty’ and ‘misleading’ forms of recognition are often disengaged from genuine expressions of political fairness.
The questions around recognition and justice have been the subjects of political and academic debate for some considerable time. In the academic setting, German sociologist Axel Honneth and American philosopher Nancy Fraser have made inspiring contributions on the concept of recognition in the context of discussions about its meaning and significance.
Recognition has been linked to redistribution and both concepts have been described as central dimensions of justice. While redistribution is the framing principle for how economic means and resources should be distributed between individuals and groups within a population, recognition stands for the majority’s readiness to confirm and show respect for a particular, traditionally marginalized group in the community.
In a widely cited article in the New Left Review (1995), Nancy Fraser demonstrates the dimensions of injustice on the example of different groups and the oppression to which they are subjected.4 One form of injustice that characterizes class-based social structures is the skewed distribution of resources, while the lack of recognition is typically inflicted on sexual minorities.
Unsurprisingly, these dimensions of injustice are often inter-connected. The working class can be subjected to a lack of cultural recognition, while discrimination against sexual minorities can be expressed in terms of financial disadvantage: difficulty finding jobs or somewhere to live. In Fraser’s analysis, the actual basis for injustices done to working class people and sexual minorities are quite distinct however – although there may be some overlap in how they are expressed.
This is in contrast to sexist and racist attitudes generally which, as Fraser explains, entail material as well as cultural discrimination, but are closely fused. In recent years, Fraser has further developed her theory of justice, adding ‘representation’ as an essential dimension of fairness within the framework of political decision-making. Arguably, however – where illness, health and sustaining life are concerned – what matters most is the relationship between redistribution and recognition.
We live in an era of recognition. The political left has repeatedly failed to motivate the electorate to commit to projects that could ensure a fair distribution of resources. Global inequality has been increasing at a rate beyond all control and has reached glaring proportions.
In present-day politicized discourse, redistribution of wealth resonates far less than recognition based on market-oriented, established traditions of justice. These forms of recognition provide contexts that make it easier for businesses to run politically slanted projects, either to express views held by the bosses, or to give a company the right profile among attractive consumer groups.
Such projects can also serve to distract attention away from bad practice and injustices linked to production, labour conditions or management behaviour. When applied in this way, the recognition of certain political issues can also be abused to obscure insight into physical realities.
Although Refugees Welcome, Me Too and Black Lives Matter have all been caught up in nets cast by various businesses and introduced into marketing campaigns, it is arguable that the most common subjects of commercialized recognition are now sexual minorities. Stunts like rainbow-washing the company logo every June are relatively inexpensive, compared with other ‘fairness projects’. Instrumentalized recognition is a meaty bone thrown to distract minority groups from demanding fair treatment in an unfair world.
Powerful politicians also like to make a point of recognizing sexual minorities, often as part of commercial initiatives or in forms interwoven into rhetoric about ‘how we in the West do things’. During Stockholm Pride Week in 2014, Mona Sahlin – former leader of the Swedish Social Democratic Party – officiated at marriages of gay couples in a branch of Seven-Eleven in Stockholm. Two years later, Ebba Busch raised her rainbow banner during a Pride Parade. This was an unexpected sight since, as leader of the Christian Democrats, she heads a parliamentary party that has voted against registered partnerships, same-sex marriages and adoptions. In Europe, even right-wing nationalist parties have come out in favour of recognition policies, as described by public speaker and writer Anna-Maria Sörberg in her important book Homonationalism (2017).5
In these cases, recognition becomes part of an explicit identity project: it includes sexual minorities in the concept of ‘we westerners’ and excludes ‘others’ while also singling them out as external threats. In previous nationalist projects, women have often been talked up as a group in need of protection. In these later variants, however, the emphasis is on defending people belonging to sexual minorities from the supposed intolerance of migrants, notably Muslims.
This kind of policy statement has emerged as an unmistakable trend in recent years – there are plenty of examples in countries such as France, the Netherlands or Sweden. More recently, though, there have been signs indicating that ‘homonationalism’ is on the way out and that, once again, homophobic utterances are viewed as acceptable in conservative and nationalistic circles. The apparent recognition shown to gay people previously was no more than a strategic self-promoting move. One depressing but likely consequence might be that other parties adjust their agendas and endorse a revivalist, explicitly homophobic subtext.
The fact that our contemporary recognition of sexual minorities has come to reflect commercial vacuity and nationalist opportunism points to possible future cracks in the façade. If issues of recognition were that easily appropriated by assorted interests, surely it would be as easy to reject them when they are no longer fit for purpose?
The requirement that recognition must come from others is the one weakness of genuine recognition politics. It diminishes its potential to bring about lasting justice for traditionally persecuted groups. Those who wish for recognition become dependent on unrelated social groups which, for more or less self-serving reasons, make such issues their own.
This may be a temporary state of affairs but the effect is that the dependent groups have to find a balance between strategies. What types of recognition should they reject? And which forms should be accepted in order to build pragmatic alliances with political opponents?
Many of us are determined not to be used as gambling tokens in some kind of nationalistic policy game. We sigh wearily at the rainbow-patterned paper mugs in high street cafés, because we see these marketing ploys as typical of how companies capitalize on our battle for freedom. Nonetheless, it is less self-evident that we should distance ourselves from signs that mainstream political groups are giving recognition to sexual minorities.
Instagram posts showing politicians cheerfully waving rainbow flags during Pride Week are written off as populist tricks by the cynics among us. But one day, we may all look back at a time when politicians of different persuasions agreed to recognize sexual minorities, and ask ourselves if things were not better then.
The fact that sexual minorities have insisted on joining institutions with heterosexual traditions, such as marriage or military service, has been decried as no better than counter-productive assimilation. It downgrades our liberation struggles, critics say. Analytically-minded academics who question such efforts as ‘a waste of our subversive potential’ are of course making a valid point. But when the argument is applied to society at large, its limitations become obvious.
Inclusion into community projects is precisely the kind of long-awaited recognition that sexual minorities have been striving to achieve. They have long been disparaged and have very good reasons for seeking inclusion: recognition can mean the difference between life and death. This was particularly true in the years of the AIDS pandemic.
Today, in view of the uncertain future and the fragility of social recognition, we must face up to the demanding but essential task of making distinctions between politically defensible alliances and hands that appear to reach out to us but, on closer scrutiny, might draw us down into a deep and destructive abyss.
In spring 2020, as the pandemic struck, a Swedish Facebook group called for people to ‘clap for our carers from a window or balcony for one minute every evening, at 20.00 hours’. The movement quickly recruited over 250,000 supporters. As coronavirus infections persisted, it is easy to understand why this gesture of appreciation to care staff grew and spread world-wide, along with other initiatives showing our gratitude to the many, often disregarded, groups of workers who have continued to look after the rest of us.

Photo by Daniel Capilla, CC BY-SA 4.0, via Wikimedia Commons.
Clearly, we are dealing with another kind of recognition here, formulated on premises different from those of the recognition of sexual minorities. Nancy Fraser begins her 1995 article with the observation that public opinion has come to see lack of cultural status as the most significant feature of discrimination. This has replaced economic exploitation as the fundamental injustice in a post-socialist world.
As social awareness of culturally based discrimination has grown, political battles for justice have focused on cultural recognition rather than financial redistribution. In its early stages, balcony applause was accompanied by concerned exchanges: would this overwhelming recognition remain hollow and fail to spur the redistribution of economic resources?
‘Clapping for carers’ is a well-meaning gesture, but obviously costs nothing until it translates into a discussion of how best to divert cash into care. It is difficult to estimate the level of true participation in the movement. Was there, perhaps, more applause on editorial pages and social media than from actual windows and balconies?
Public celebrations of care have suited employers and people in power well by offering an escape route from the distribution of greater financial rewards to hard-pressed groups of care workers. This represents a complex set of issues which political and business leaders dislike tackling. No wonder that many of them, even those with no previous record of backing the rights of care staff, joined the chorus of no-cost approval.
Perhaps the balcony applause during the spring of 2020 is the equivalent of the empty recognition that fills a rainbow-coloured coffee mug? A pat on the back, a thank-you for praiseworthy work and no more than that?
The health and social care workers who were ‘clapped for’ from real and digital balconies are mostly women on low pay. Replacing financial remuneration with empty recognition has, of course, been a constant feature in the employment of care staff. Perhaps this is to make up for the fact that their work has long been regarded as a female ‘calling’ rather than a profession with responsibility for life and death.
Recently, nurses in Sweden have managed to increase their income. However, past experiences of pandemic pressures have made it clear that they, like other professions in the care sector, need redistributions that affect more than their wage packets. They urgently require resources that will provide decent work environments, as well as relief from obligatory overtime and the loss of holiday entitlements.
A state of emergency has become a near-permanent rule in the caring professions, and staff work in conditions that would never have been accepted by most other professional groups. The fact that recognition of the caring professions has never resulted in improving their working environment might be because they are seen, for many reasons, as belonging to a special sector.
When, towards the end of March 2020, the Swedish Civil Contingencies Agency released a list of socially essential jobs, we were at last given a clearer idea of which workers we really depend on.6 The list was intended to offer a guideline for allocating rights to childcare, in case the pandemic led to the closure of schools and nurseries. It included jobs in energy supplies, transport, trade, local authority technical management and, naturally, health and social care. So far, so straightforward.
The big question now is how much this recognition from a state-controlled authority will, in years to come, affect wage negotiations. It is true that, in certain cases, trade unions have managed to turn recognition into something of more substantial value. One public sector trade union leader, Tobias Baudin, has said he is pleased with an agreement reached in November 2020, covering 400,000 workers in schools, and in health and social care.
Other groups have done less well. The Swedish Care Union is bound by an agreement that is up for re-negotiation in 2022. Meanwhile, there have been rumblings of discontent from the corresponding sector in Norway. Quite reasonably, nurses are unhappy about an agreement reached in September last year, which gives them a monthly increase of about €5 after tax. As one nurse said in an interview: ‘Recognition is all very well, but the last time applause provided a living wage was for Roman gladiators in the Colosseum’.7
The coronavirus pandemic has brought with it many examples of empty recognition. But have last year’s policies left us with other, darker outcomes for the future? In July 2020, Amnesty International published a world-wide record of death statistics among health care workers.8 This was followed by articles, appearing almost daily, which reported on the large numbers of care staff infected with COVID-19 who were falling ill and, often, dying. In addition, Amnesty also collected data from different countries, including the United Kingdom, showing that a comparison of entire populations in age bands reveals that some groups of workers have higher mortality rates. These include taxi drivers and public transport staff, factory workers and security guards. Access to personal protective equipment (PPE) has been a critical factor, particularly in the early stages of the pandemic, but when social and health care staff were urged to come to work without being guaranteed adequate PPE, matters were clearly turning dangerous. Serious questions had to be asked. Lisa Pelling, chief analyst at the Stockholm-based think tank Arena Idé, has compiled a report based on questionnaire and interview responses by members of the Swedish Municipal Workers’ Union. Pelling’s report shows how the pandemic, and the political decisions made as it progressed, have made Sweden’s class structure more evident.9 Improved state backing for sick pay has been an important intervention, allowing employees with permanent contracts to stay at home in case of illness. Temporary workers do not benefit, however. In Spring 2020, lack of PPE for doctors and registered nurses was dealt with sooner than for associate nurses and other support staff, who had no option but to arrive at work wearing bin bags, privately bought diving masks and face shields cobbled together from overhead projector acetates. How did we come to this? Could it have anything to do with recognition politics?

COVID-19 emergency response activities, Sajida Foundation hospital’s isolation Center, Narayanganj, Dhaka, Bangladesh.
Photo by UN Women Asia and the Pacific from Flickr
Celebrating ‘our heroes’ on balconies or on the smartly edited social media accounts of the powerful turned out to be wholly compatible with ignoring the interests of care staff and failing to protect them from risk. The chorus of praise transformed health workers into idealized figures isolated from the self-image of the majority. This is in stark contrast to the kind of recognition that aims to integrate a traditionally marginalised group into the social context. It goes without saying that many have experienced intense grief at the loss of parents, partners, friends, colleagues and others who worked within health and social care – all of them people we can recognize as ‘ourselves’. This form of recognition manifests itself in parallel with another narrative, however: the story of a respected group separate from the rest of us. It follows that the loss of some of its members, though saddening, is more bearable than losing someone we regard as ‘one of our own’. This distancing mechanism makes the applause part of a global narrative in which health care staff and other workers performing socially essential tasks are presented as warriors in a perilous battle fought against a mighty and invisible enemy. We acknowledge their praiseworthy heroism but at the same time refuse to give them the recognition that would make their deaths unacceptable. War metaphors have become common currency in the past year, perhaps to help drum up a nationalist fighting spirit among civilians and promote a tale that suits political ends. Creating an image of the virus as an independent engine of death, with inherent intentions and agency, helps distract people from any lack of provision and planning at the national level, and from errors in managing the spread of infection. When health care staff are seen as soldiers fighting at the front – as in the Swedish TV documentary ‘Tales from the Front Line’ or, implicitly, in the widely used English phrase ‘frontline workers’ – deaths seem honourable but also somehow tolerable. Nonetheless, those who consider the death of soldiers on the battle field unavoidable may perhaps find it less acceptable that health care workers die because they lack PPE. They may have been recognized as heroes by the public, by politicians, princes and princesses, but they risk being sacrificed for the privilege.
Lack of recognition can have fateful outcomes, so can empty or misleading forms of acknowledgement. The high mortality rate among gay men during the AIDS crisis, and deaths among health care workers related to COVID-19, reflect different forms of recognition. Homosexual men died from the consequences of HIV because society at large didn’t recognize them as worthy of protection. Health care workers continue to die after contracting the coronavirus because the recognition they receive has set them up as expendable. Whenever people die from causes we are in a position to control, recognition matters a great deal – especially as it is often linked to redistribution of funds. Lack of recognition slows research, prevents the funding of effective systems to deal with the spread of infections, and blocks effective collaboration between the clinical professions and political activists. The fight to achieve recognition of the value of gay lives in the wake of the AIDS crisis reminds us of well-documented activism in the USA which, in the end, contributed to a change in political attitudes. Similar activism was also at work in Nordic welfare states. In her important study of Nordic legislation about venereal disease, historian Ida Blom has described how, in parallel with the AIDS crisis, welfare states modified their responsibility to keep society healthy by backing a new strategy that shifted the burden of disease prevention onto individuals and potentially exposed groups.10 The roles of such groups in the politics of recognition has also been discussed by physician and medical historian Ketil Slagstad in an article about AIDS activism in Norway.11 Slagstad demonstrates convincingly that, if the fight on behalf of AIDS sufferers is to be properly understood, it must not be thought of as a reaction to conservative unwillingness to face up to issues arising from HIV and AIDS. Rather, the fight developed before the AIDS crisis, as an extension of a more far-reaching struggle for equal access to health care for sexual minorities. Similar arguments emphasize the importance of ensuring that recognition of health care staff during the coronavirus crisis becomes established in a wider context. After all, there have been enduring efforts to organise better conditions for health and social care workers in the past, before the advent of the heroic narrative dominant today.
This essay has focused on two different forms of recognition along with their emerging effects and drawbacks. These have entailed disconnections between recognition and other dimensions of fairness, notably in the redistribution of resources. Some political battles have been fought and won. Consequently, in many parts of the world sexual minorities now enjoy unbiased recognition and near-to-full social inclusion. However, recent examples of hollow and misleading forms of recognition of sexual minorities must also be noted. ‘Pink-washing’ and rainbow advertising campaigns can often be identified as cases of ‘empty’ recognition. The homonationalistic trend that pays lip-service to tolerance of sexual minorities, and makes it part of the political agenda, stands out as seriously misleading. These two dimensions of recognition also relate to previously overlooked groups of workers in the health and social care sectors, and entails praising them for their contribution to the nationwide task of coping with the pandemic. Applause from windows and balconies is a well-earned tribute to people who have dedicated themselves to helping the rest of us survive a frightening time. However, the false notes sound loud and clear when the authorities, whose actions have hitherto led to reduced resources for health and social care, suddenly join in the chorus of praise. Because care staff have been left a political legacy of under-financing, the burst of official enthusiasm is no more than an empty form of recognition. But another dimension, even more treacherous and misleading, has now merged with the emptiness. It comes from a policy of re-prioritisation pursued in recent years that has permitted the spread of infection among health and social care workers. Bombastic verbiage, sanctioned by political authority, has created a heroic narrative in which care professionals stand on the front line of battle against an external enemy. Health care workers are cast as soldiers, prepared to make the ultimate sacrifice. This officially endorsed story serves as a useful diversion from having to admit political responsibility. The fact that health workers do fall ill, often fatally, is of course due to resource-poverty. It is hard to predict what forms of recognition policy the pandemic will bring next. We live in a time of recognition, but what that will mean in the long run is far from clear. Certainly, one inescapable aspect of recognition is its fragility. A discussion on the dimensions and effects of recognition, in the context of real outcomes, is bound to be of value and may offer hope of achieving greater fairness in times of pandemic.
Toyin Owoseje, “Corona virus is ‘the great equalizer’ Madonna tells fans from her bathtub”, in CNN Entertainment, 23 March 2020
Joseph Bennington-Castro, “How AIDS remained an unspoken – but deadly epidemic for years”, History, 1 June 2020
Nancy Fraser, ‘From redistribution to recognition? Dilemmas of justice in a “post-socialist” age’, New Left Review, 1/212, 1995
Anna-Maria Sörberg, Homonationalism, Leopard förlag, 2017
Myndigheten för samhällsskydd och beredskap [The Swedish Civil Contingencies Agency], Guidelines for child care by a caregiver in a socially essential post, MSBFS, 3/2020
Synnøve Sundby Fallmyr, and Elin Åsbakk Lind, “Lønnsoppgjøret for sykepleierne: rett og slett begredelig” [Income settlement for nurses: simply deplorable], NRK (Norwegian Broadcasting Corporation), 16 September 2020
Lisa Pelling, Att stå längst fram. En skildring av villkoren för medlemmar i Kommunal under coronakrisen våren 2020 [On the front line. An account of the conditions of work for local authority workers during the corona crisis in spring 2020], Arena idé, Stockholm, 2020
Ida Blom, Medicine, Morality, and Political Culture. Legislation on venereal disease in five northern European Countries, c. 1870- c.1995, Scandbook, 2012
Ketil Slagstad, “The amphibious nature of AIDS activism: Medical Professionals and Gay and Lesbian Communities in Norway, 1975–87”, in Medical History, Vol. 64, 3/2020
Published 27 March 2021
Original in Swedish
Translated by
Anna Paterson
First published by Ord&Bild 5/2020
Contributed by Ord&Bild © Karl Gauffin / Ord&Bild / Eurozine
PDF/PRINT
After over 20 years of publishing for free, Eurozine needs your support to get through an exceptionally lean year.
Become a Patron and get exciting perks for your help!
![]()

Want to hear a human voice?
Listen and subscribe wherever
you get your podcasts.
Subscribe to know what’s worth thinking about.
Why was the distinguishing mark of female genitalia erased from NASA’s 1970s image travelling outer space? And will compromised depictions of life on Earth avoid sexist, racist and anthropocentric simplifications by 2036?

While book publishing is an ailing industry, children’s books are booming. But political attacks and censorship are also threatening this thriving sector.